 Infertility Counselling
Infertility Counselling Female Infertility Treatment
Female Infertility Treatment Andrology Treatment
Andrology Treatment Fertility Enhancing Surgeries - Female
Fertility Enhancing Surgeries - Female Fertility Enhancing Surgeries - Male
Fertility Enhancing Surgeries - Male Endoscopy Treatment
Endoscopy Treatment IUI Treatment
IUI Treatment IVF Treatment
IVF Treatment ICSI Treatment
ICSI Treatment Advanced IVF Solutions
Advanced IVF Solutions Embryology
Embryology Vitrification Egg, Embryo, Sperm Freezing
Vitrification Egg, Embryo, Sperm Freezing Preimplantation Genetic Testing (PGT)
Preimplantation Genetic Testing (PGT) Donation Program Embryo / Egg / Sperm
Donation Program Embryo / Egg / Sperm
Intrauterine Insemination, In Vitro Fertilisation, Laser-Assisted Hatching and finally pregnancy

Mrs. SB, who was 35, and her partner lived a happy and lovely life for 6 years. The couple were trying to become parents but in vain.
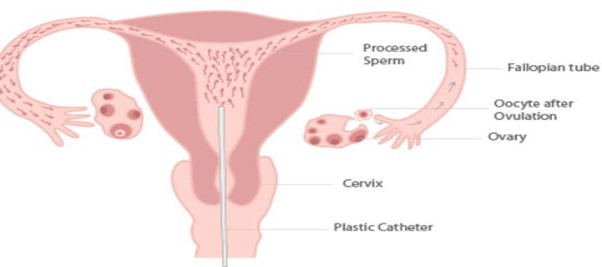
Mrs. SB suffered from primary fertility, that is, never achieved pregnancy or succeeded in carrying it to full term. She went to a fertility centre elsewhere to continue her infertility treatments. 3 intrauterine insemination procedures (IUI, a simple procedure in which sperm is placed directly into the uterus, allowing healthy sperm to reach closer to the egg) were attempted but failed.
The couple came to Nova IVF Fertility Centre, Kolkata, hoping to continue their fertility treatments under the supervision of the fertility specialist Dr. Suparna Bhattacharya. Following the examination, she advised Mrs. SB to have some basic fertility assessments. She had a normal BMI and had previously undergone diagnostic hystero-laparoscopy (diagnostic HL, a method of evaluating conditions associated with infertility in the female reproductive organs) following three failed IUI cycles.
According to the findings, the laparoscopy was normal, with flimsy adhesions and patent tubes. An endometrium TBPCR (to confirm TB) was performed to diagnose female genital tuberculosis, a common cause of infertility, but the results revealed no signs of infection. Her vital signs were normal, and her abdomen’s examination revealed that it was soft and non-tender.
She has a normal cervix with no erosion on P/S examination. Her first ultrasonography (USG, a diagnostic imaging technique that uses sound waves to look at organs inside the body) revealed a normal uterus with an adherent ovary on the left and with normal ovary on the right.
Antral follicle count (AFC, a non-invasive test used to assess a woman's ovarian reserve, that is, the number of eggs contained in her ovaries at a given time) values are 6-7 on both sides, with a 2-cm endometriotic cyst in the left ovary. Her anti-Mullerian hormone (AMH, an indicator that provides information about the number of ovarian follicles in a woman) level was 2.8 ng/ml, and her husband's sperm analysis was normal.
After a thorough clinical assessment, she was counselled about IUI and informed of the procedure's benefits and limitations, as well as her age factor, and the following treatment options were suggested IUI for 1-2 cycles and self-IVF (a process in which the matured own eggs are retrieved from a woman’s ovary and combined with her partner’s sperm outside the body to form embryos.
She agreed to the treatment plan and underwent one cycle of IUI followed by IVF. However, she did not conceive in the cycle and went for IVF in the next cycle.
In her next menstrual cycle, she was stimulated with injections and 11 oocytes were retrieved from her uterus. After vitrification (an advanced cryopreservation technique for embryos that involves dehydrating them in solution before rapidly freezing them), 3 healthy blastocysts yielded. Following the second cycle, endometrial preparation was done.
Endometrial preparation
To begin, the uterine endometrium is the lining of the uterus that is responsible for embryo implantation. To block the natural hormone regulation and gain some control over her period, a woman will need to undergo endometrial preparation using GnRH analogues. Oral contraceptive pills (OCPs) are considered another option.
The woman was then prescribed a treatment consisting of oral or patched oestrogen. In addition, about 3-5 days before the embryo transfer, progesterone should be administered, either in a pill or vaginal egg form.
2 quality blastocysts with adequate luteal phase ( (the female cycle period that begins with ovulation and ends with embryo implantation during fertilisation) support were transferred via frozen embryo transfer (a process uses embryos that have been previously cryopreserved and thawed for the procedure). She was not able to become pregnant.
Her clinical case was reviewed again, and she was advised to undergo thrombophilia profile testing (to identify people who are at an increased risk of pregnancy complications due to hereditary or acquired thrombophilia), which revealed no abnormalities. Her 3D cavity scan also showed a normal cavity.
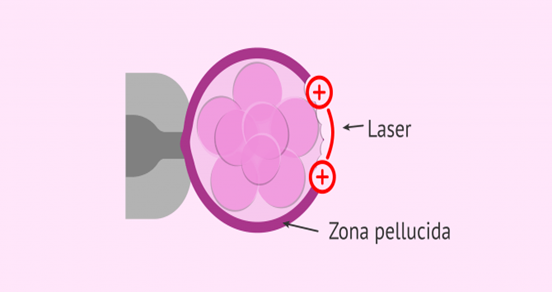
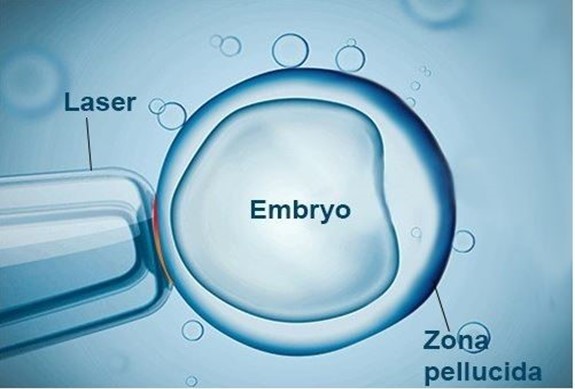
The lab tests confirmed that the sperm profile was normal, and that the remaining blastocytes were of a healthy grade. After downregulating with an injection on day 21 of the previous cycle, the endometrium was carefully prepared again, and the frozen transfer was performed. Then, laser assisted hatching (LAH, a process involves refining of the zona pellucida the glycoprotein layer that protects embryos from the outside environment so that they can emerge and implant in the future mother's womb when the time comes) were performed on the transferred embryo and adequate luteal phase support was provided, one quality blastocyst was transferred.
After 10 days of egg transfer, her HCG was 323 Miu/ml. Finally, she had an uneventful pregnancy at 27 weeks.
Conclusion
Nova IVF had left no stone unturned to ensure a successful outcome. Our team of fertility specialists, embryologists, fertility-trained nurses, and counselors work as a team to help couples build families.













Add new comment